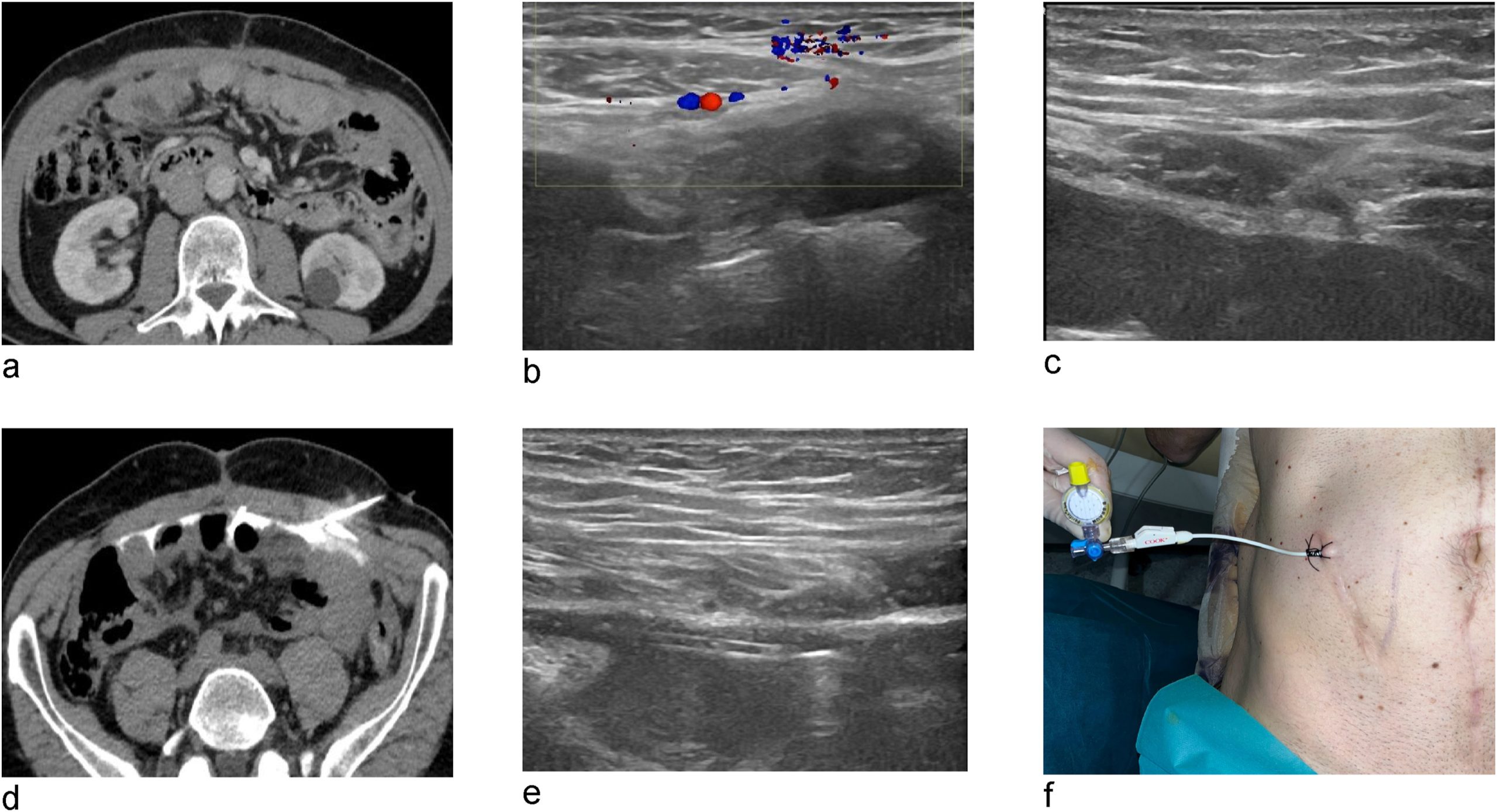
Approximately 4% to 5% of patients with peritoneal carcinomatosis present with severe adhesions (dense, rigid scar tissue that causes organs to stick to each other and to the abdominal wall) as a result of previous surgical interventions.
This anatomical blockage creates a "non-accessible abdomen," making the introduction of surgical instruments (trocars) carry an unacceptable risk of bowel perforation. Until now, facing this situation meant automatic exclusion from targeted chemotherapy options, leaving these patients unable to benefit from PIPAC or ePIPAC.
The procedure is performed under propofol sedation and intravenous antibiotic prophylaxis to ensure the patient experiences no discomfort.
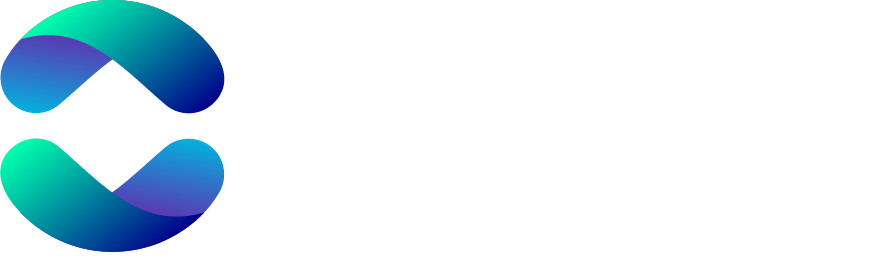
Interventional radiologists identify the safest and most precise entry point on the abdominal wall in real time, strictly avoiding the epigastric blood vessels and tumor implants.
A millimetric needle is introduced to inject a mixture of saline solution and contrast media. This fluid gently separates the tissue layers, creating a small, safe "artificial pocket" of approximately 100 mL.
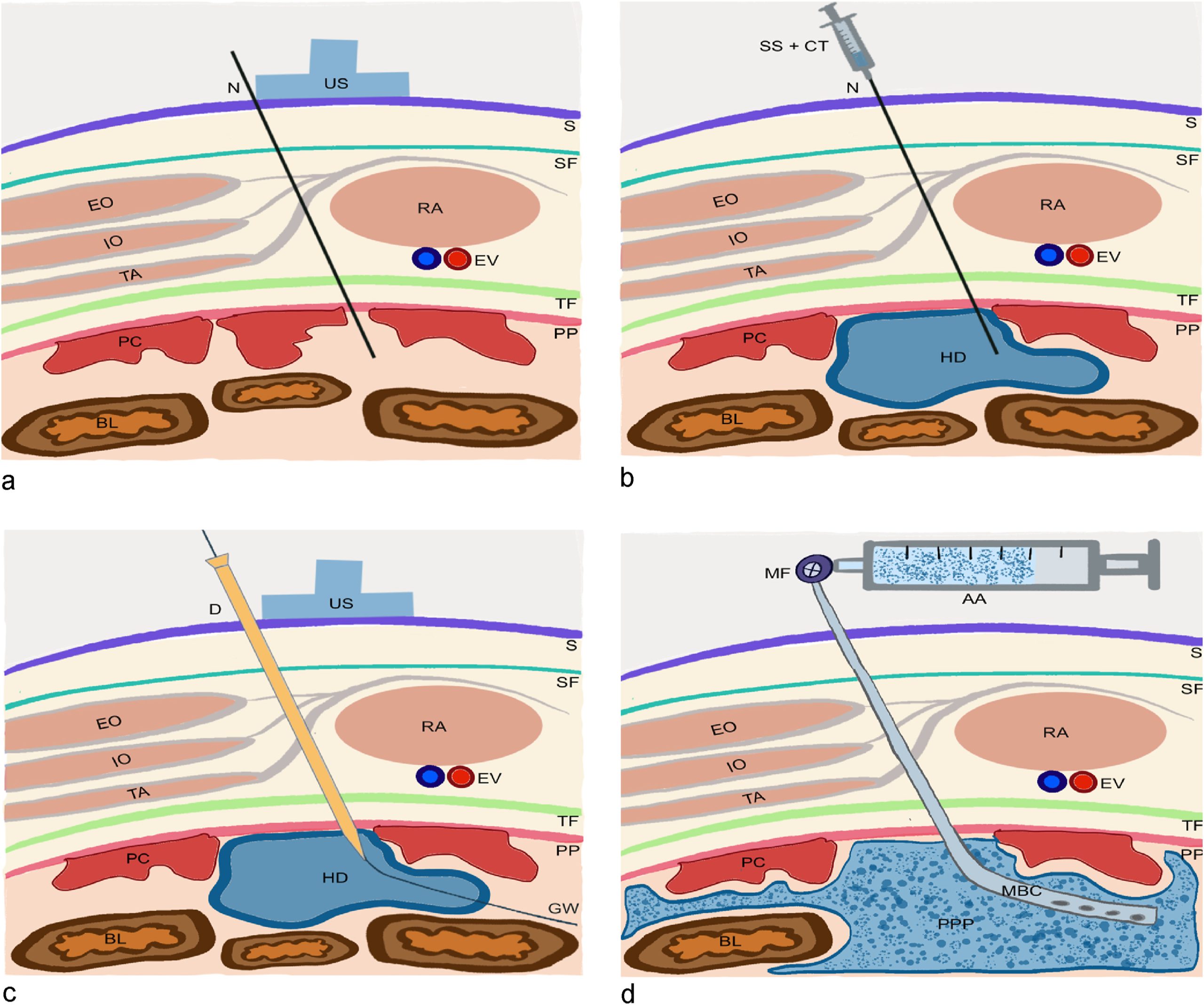
A very fine drainage catheter (8.5 French) equipped with an antibacterial filter is positioned within this protected space. A minimal initial air volume of 100 to 200 mL is insufflated, and correct placement is confirmed via a control CT scan.
Over a mean of 5.5 days (ranging from 4 to 7 days), 250 to 500 mL of filtered air is intermittently introduced through the catheter each day.
The process continues until an accumulated volume of 1 to 3 liters of air is reached, always tailored to the patient’s physical tolerance.
Medical staff assess the patient daily to monitor for any adverse symptoms, such as significant pain, respiratory distress, or nausea.
Once a minimum volume of 1 liter of air is reached, the patient is ready for surgery. On the day of the PIPAC procedure, a CT scan is performed to verify that the adhesions have elongated and that there is sufficient pneumatic space to operate with 100% safety.
In all patients treated at IVOQA who initially presented with a non-accessible abdomen, optimal and safe laparoscopic access was successfully achieved.
Thanks to the space gained through PPP, a total of 13 aerosol chemotherapy procedures (PIPAC and ePIPAC) were effectively delivered to individuals who previously had zero options to receive them.
No medical complications or adverse side effects of any grade were recorded from either catheter placement or air insufflation, proving to be an exceptionally safe and well-tolerated method for oncology patients.





